
Special Populations

Ryan McGrath, PhD
Assistant Professor
North Dakota State University
Fargo, North Dakota, United States
Samantha FitzSimmons
Graduate Assistant
North Dakota State University
Fargo, North Dakota, United States
Sarah Andrew
Undergraduate Assistant
North Dakota State University
Fargo, North Dakota, United States
Kennedy Black
Undergraduate Assistant
North Dakota State University
Fargo, North Dakota, United States
Bryan K. Christensen
Professor
North Dakota State University
Fargo, North Dakota, United States
Jacob Kieser
Undergraduate Assistant
North Dakota State University
Fargo, North Dakota, United States
Matthew Langford
Undergraduate Assistant
North Dakota State University
Fargo, North Dakota, United States
Kyle J. Hackney
Associate Professor
North Dakota State University
Fargo, North Dakota, United States
Muscle weakness, which is often determined with low handgrip strength (HGS), is associated with several adverse health conditions during aging, however, the prevalence of weakness in the United States is not well-understood.
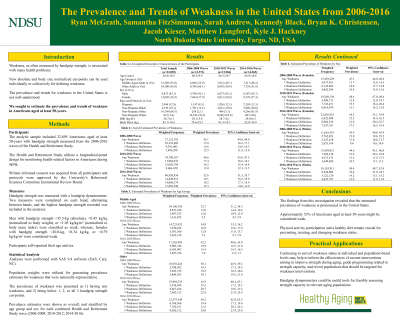
Purpose: We sought to estimate the prevalence of weakness in Americans aged at least 50-years.
Methods: The total unweighted analytic sample included 22,895 Americans from the 2006-2016 waves of the Health and Retirement Study. HGS was measured with a handgrip dynamometer. There were two HGS measurements performed on each hand and the single highest HGS recorded was included in the analyses. Males with weakness were below at least one of the absolute or normalized (body mass, body mass index) cut-points: < 35.5-kg, < 0.45-kg/kg, < 1.05-kg/kg/m2. The presence of any weakness in females was also identified as being below one of the absolute or normalized HGS cut-points: < 20.0-kg, < 0.34-kg/kg, or < 0.79-kg/kg/m2. Survey weights were utilized to generate weakness prevalence estimates that were nationally-representative. Separate multilevel logistic regression models examined trends in any weakness for the overall sample and by sub-groups.
Results: The overall prevalence of weakness was 45.1% (95% confidence interval (CI): 44.0-46.0) in the 2006-2008 waves, 46.6% (CI: 45.6-47.5) in the 2010-2012 waves, and 52.6% (CI: 51.5-53.7) in the 2014-2016 waves. Weakness prevalence was higher for older Americans (64.2%; CI: 62.8-65.5) compared to middle-aged Americans (42.2%; CI: 40.6-43.8) in the 2014-2016 waves. Moreover, the prevalence of weakness in the 2014-2016 waves was higher in females (54.5%; CI: 53.1-55.9) than males (50.4%; CI: 48.7-52.0). Differences existed in weakness prevalence across races and ethnicities over the study period.
Conclusions: Our investigation found that up to 53% of Americans aged at least 50-years were weak. Physical activity participation, especially resistance training, and dietary counseling remain crucial for preventing, treating, and reversing weakness status. Continuing to surveil the trends in weakness status may help to inform the effectiveness of current interventions aiming to improve strength during aging, guide programming related to strength capacity, and reveal populations that should be targeted for weakness interventions. Such surveillance may help the rapidly growing older American demographic live longer and with more independence. PRACTICAL APPLICATIONS: Handgrip dynamometers could be useful tools for feasibly assessing strength capacity in relevant aging populations. Guidelines for appropriate physical activity participation to improve strength in older adults should be greatly encouraged for preventing and treating weakness. Nutritional counseling is also advised as nutrient intake may influence health and responses to interventions. Repeated measures of HGS could be used for monitoring progress, but changes of functional abilities may inform how strength assessments are conducted.
Acknowledgements: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R15AG072348. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.