
Resistance Training/Periodization

John Lawson
Master's Student
University of Central Florida
Orlando, Florida, United States

Christopher E. Proppe, MS, LAT, ATC, CSCS
PhD Student
University of Central Florida
New Smyrna, Florida, United States
 photo")
Paola M. Rivera, MS (she/her/hers)
PhD Student
University of Central Florida
Orlando, Florida, United States
David Gonzalez Rojas
Professor
University of Central Florida
Orlando, Florida, United States
Shane hammer
Assistant Professor
Oklahoma State University
Stillwater, Oklahoma, United States
Michael A. Trevino, PhD
Assistant Professor
Oklahoma State University
Stillwater, Oklahoma, United States

Taylor K. Dinyer-McNeely, PhD
Assistant Professor
Oklahoma State University
Stillwater, Oklahoma, United States

Tony R. Montgomery, Jr., PhD
Graduate Student
Oklahoma State University
Stillwater, Oklahoma, United States

Alex Olmos, MS
Graduate Student
Oklahoma State University
Stillwater, Oklahoma, United States
Kylie Burleson
Graduate Student
Oklahoma State University
Stillwater, Oklahoma, United States

Haley C. Bergstrom, PhD, CSCS*D
Associate Professor
University of Kentucky
Lexington, Kentucky, United States

Pasquale J. Succi, Jr., MS, CSCS
Graduate Student
University of Kentucky
Lexington, Kentucky, United States
Joshua L. Keller
Assistant Professor
University of South Alabama
Mobile, Alabama, United States

Ethan C. Hill, PhD, CSCS, EP
Assistant Professor
University of Central Florida
Orlando, Florida, United States
Purpose: The general recommendation for blood flow restriction (BFR) exercise suggests using an arterial occlusion pressure (AOP) of 40-80%. For BFR protocols, training load is typically prescribed relative to maximal strength under non-restricted conditions. BFR at a high AOP ( >100%) may acutely increase maximal strength, but the effect of a commonly used moderate AOP on maximal strength is not known. Therefore, the purpose of this study was to examine the acute effects of BFR applied at 60% of AOP on maximal strength.
Methods: Ten (mean age ± SD; 21.4 ± 1.3 years) females who regularly (at least 2x/week for the past 6 months) performed resistance exercise completed maximal unilateral isometric and concentric leg extension muscle actions using their dominant leg with and without BFR. During the maximal strength tests with BFR, the cuff was applied and inflated immediately prior to each repetition and deflated after each repetition. The isometric muscle actions were performed at a knee joint angle of 65° and sustained for 5 seconds, whereas the concentric muscle actions were performed at an angular velocity of 90°·s-1 through a full 90° range of motion. Participants visited the laboratory twice to complete three repetitions of each muscle action, both with and without BFR (four randomized sets of three repetitions each visit). For each set, the highest torque value produced was used for further analyses. Test-retest reliability for concentric and isometric maximal strength was assessed between visits and the model 2,1 was used to calculate the intraclass correlation coefficients (ICC). A 2(Condition [BFR, no BFR]) x 2 (Visit [1, 2]) x 2 (Mode [Concentric, Isometric]) repeated measures ANOVA was used to examine mean differences in maximal strength.
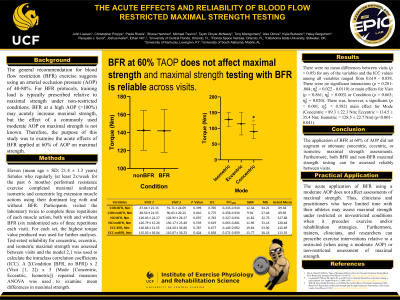
Results: There were no mean differences between visits (p > 0.05) for any of the variables and the ICC values among all variables ranged from 0.773 - 0.931. There were no significant interactions (p = 0.372-.927; ηp2 = 0.001 - 0.089) or main effects for Visit (p = 0.837; ηp2 = 0.005) or Condition (p = 0.588; ηp2 = 0.034). There was, however, a significant (p < 0.001; ηp2 = 0.895) main effect for Mode (Concentric = 89.3 ± 22.3 Nm; Isometric = 128.5 ± 22.7 Nm). Conclusion: The application of BFR at 60% of AOP did not augment or attenuate concentric or isometric maximal strength assessments. Furthermore, both BFR and non-BFR maximal strength testing can be assessed reliably between visits. PRACTICAL APPLICATIONS: The acute application of BFR using a moderate AOP does not affect assessments of maximal strength. Thus, clinicians and practitioners who have limited time with their athletes may assess maximal strength under restricted or un-restricted conditions when it precedes exercise and/or rehabilitation strategies. Furthermore, trainers, clinicians, and researchers can prescribe exercise interventions relative to a restricted (when using a moderate AOP) or non-restricted assessment of maximal strength.
Acknowledgements: None