
Resistance Training/Periodization
 photo")
Cade Carter (he/him/his)
Student
Coastal Carolina University
Myrtle Beach, South Carolina, United States
Timothy R. Rotarius
Assistant Professor
Coastal Carolina University
Conway, South Carolina, United States
Justin P. Guilkey
Assistant Professor
Coastal Carolina University
Conway, South Carolina, United States
Jakob D. Lauver
Assistant Professor
Coastal Carolina University
Conway, South Carolina, United States
A traditional blood flow restriction (BFR) exercise protocol consists of 1 x 30 repetitions, followed by 3 x 15 repetitions, with 1 minute of recovery between each set. However, there is little evidence to suggest that this traditional protocol is the only choice for BFR training.
Purpose: The purpose of this study was to compare the acute physiological responses of various blood flow restriction protocols to the traditional BFR protocol.
Methods: Healthy adults (26 ± 8 yrs) who were currently physically active participated in this study. Participants reported to the Integrated Exercise Science laboratory on 5 separate occasions. Visit 1 consisted of a 1-repetition maximum (1-RM) assessment of bicep curl. The remaining visits consisted of 1 of the 4 randomized experimental conditions. The 4 experimental conditions were as follows: Traditional BFR (TRAD-BFR) consisted of 1 x 30 repetitions followed by 3 x 15 repetitions with 1 minute of recovery between each set; Modified Time BFR (MT-BFR) consisted of 1 x 30 repetitions followed by 3 x 15 repetitions with 2 minutes and 40 seconds of recovery between each set; Modified Sets BFR (MS-BFR) consisted of 1 x 15 repetitions followed by alternating sets of 7 and 8 repetitions, with 1 minute of recovery between sets; Modified Time and Sets BFR (MTS-BFR) consisted of the 1 x 15 repetitions followed by alternating sets of 7 and 8 repetitions with 40 seconds of recovery between the 1st and 2nd set, and 20 seconds of recovery between each subsequent set. Each condition was completed at 30% of 1-RM and resulted in the completion of 75 repetitions of bicep curl. BFR cuffs were applied to the proximal end of each arm. Each cuff was inflated to 50% of limb occlusion pressure, which was measured at the beginning of each trial, and remained inflated until completion of each experimental condition. Near-Infrared Spectroscopy (NIRS) was used to measure oxygen saturation of the biceps brachii during each condition. Rate of Perceived Exertion (RPE) was assessed prior to exercise and following the completion of 30, 45, 60, and 75 repetitions. Lactate measurements were also recorded prior to exercise and following the completion of 75 repetitions. Two-way ANOVAs (time x condition) was utilized to assess differences.
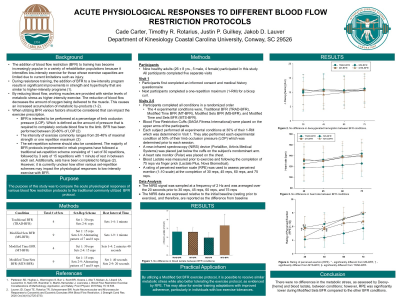
Results: Deoxygenated hemoglobin (HHb) was similar between TRAD-BFR and MS-BFR at 30 repetitions (TRAD: 10.6 ± 7.8 au, MS: 11.9 ± 5.8 au, p > 0.05), 45 reps (TRAD: 11.4 ± 6.5 au, MS: 12.3 ± 6.6 au, p > 0.05), 60 reps (TRAD: 10.5 ± 5.8 au, MS: 12.1 ± 6.0 au, p > 0.05), and 75 reps (TRAD: 10.0 ± 5.0 au, MS: 13.0 ± 5.2 au, p > 0.05). However, RPE was higher during TRAD-BFR compared to MS-BFR at 45 reps (TRAD: 6.2 ± 1.9, MS: 4.6 ± 1.1, p = 0.04), 60 reps (TRAD: 7.2 ± 1.9, MS: 5.0 ± 1.6, p = 0.01), and 75 reps (TRAD: 8 ± 1.7 au, MS: 6 ± 1.4 au, p = 0.01), there was no difference at 30 reps (TRAD: 5.6 ± 1.5, MS: 4.4 ± 1.1, p = 0.2).
Conclusion: There were no differences in the metabolic stress, as assessed by HHb, between conditions; however, RPE was significantly higher in Traditional BFR compared to Modified Sets BFR. PRACTICAL APPLICATION: By utilizing a Modified Set BFR exercise protocol, it is possible to receive the same metabolic stress while also better tolerating the exercise protocol, as evidenced by RPE. This may allow for similar training adaptations to MS-BFR with an improved adherence, particularly in individuals with low exercise tolerances.
Acknowledgements: None