
Special Populations

Lexie M. Tonnemacher
Student
Creighton University
Omaha, Nebraska, United States

Kelley G. Hammond, PhD, CSCS
Assistant Professor
Creighton University
Omaha, Nebraska, United States

Mitchel A. Magrini, PhD
Assistant Professor
Creighton University
Omaha, Nebraska, United States
Parkinson’s disease (PD) is a progressive neurodegenerative disorder affecting more than one million people in the United States. PD is characterized by tremor, postural instability, bradykinesia (slowness of movement), and muscle rigidity and weakness. Deficits in muscle activation, strength, and rate of force development contribute to motor difficulties in PD. Normal aging results in motor unit loss and reorganization (i.e., denervation/reinnervation) which contributes to sarcopenia and occurs to varying extents among older adults. Motor unit loss does not always elicit myofiber death, as some denervated myofibers are reinnervated by another local motor neuron and incorporated into that motor unit. Neural cell adhesion molecule (NCAM) is expressed by myofibers when they are denervated and need reinnervation by motor neuron of a nearby motor unit. If a myofiber fails to be reinnervated, it will undergo apoptosis (programmed cell death), which contributes to sarcopenia and associated weakness. Evaluation of myofiber size, type, and NCAM expression can provide evidence for the rate of denervation for each myofiber type, which helps to characterize PD-specific changes in motor unit remodeling.
Purpose: The purpose of this pilot study was to measure the relative expression of NCAM in healthy older adults (OLD) compared to patients with PD and identify differences in myofiber type specific NCAM expression.
Methods: Muscle biopsies from the vastus lateralis were collected from persons with PD (65 ± 9 yr, n = 7; males =3) and OLD (65 ± 14 yr, n = 2 males) using the percutaneous needle biopsy technique. All markers (NCAM and myosin heavy chain) were manually analyzed and counted using ImageJ (NIH) software. Differences (p ≤ 0.05) between PD and OLD were analyzed using two-tailed independent t-tests and effect size was calculated using Hedges g (small: g ≤ 0.19; medium: g = 0.20 - 0.79; large: g > 0.80).
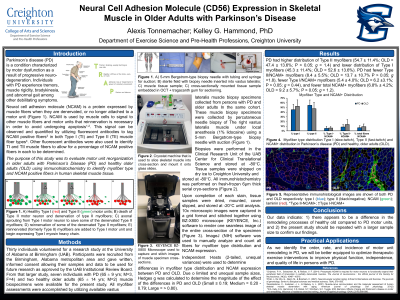
Results: There were no significant differences (p > 0.05) between PD and OLD for myofiber distribution (% Type II), total NCAM+ myofibers, or NCAM+ myofibers by type. However, PD had higher distribution of Type II myofibers (54.7 ± 11.4%; OLD = 47.4 ± 13.6%; P > 0.05; g = 1.4) and lower distribution of Type I myofibers (45.3 ± 11.4%; OLD = 52.6 ± 13.6%). PD had fewer Type II/NCAM+ myofibers (8.4 ± 5.5%; OLD = 13.7 ± 10.7% P > 0.05; g =1.8), fewer Type I/NCAM+ myofibers (5.4 ± 4.0%; OLD = 6.2 ±3.1%; P > 0.05; g = 0.44), and fewer total NCAM+ myofibers (6.8% ± 4.2%; OLD = 9.2 ± 5.7%; P > 0.05; g = 1.2).
Conclusions: Although the data should be interpreted with caution given the small sample size, there appears to be a difference in the motor unit remodeling processes in patients with PD compared to OLD. The difference in myofiber type specific NCAM expression in PD compared to OLD may lead to changes in myofiber type distribution in both groups, which could contribute to deficits in strength and rate of force development in PD. PRACTICAL APPLICATIONS: While PD is largely a central nervous system disorder, the peripheral affects (i.e., motor dysfunction) lead to a reduced quality of life and functional ability in this population. These preliminary data suggest that NCAM may be a useful biomarker to characterize the order/timing of motor unit remodeling in patients with PD, which may help identify a more precise exercise intervention point.
Acknowledgements: None