
Nutrition/Ergogenic Aids

Troy M. Purdom, PhD
Associate Professor of Kinesiology
North Carolina A&T State University
Greensboro, North Carolina, United States
Brianna Jones
Student
North Carolina Agricultural and Technical State University
Greensboro, North Carolina, United States

Marc Cook, PhD
Associate Professor
North Carolina Agricultural and Technical State University
Greensboro, North Carolina, United States
Heather L. Colleran, PhD RDN CSSD LDN CSCS
Associate Professor
North Carolina Agricultural and Technical State University
Greensboro, North Carolina, United States
Lauren San Diego
Graduate Student
North Carolina Agricultural and Technical State University
Greensboro, North Carolina, United States
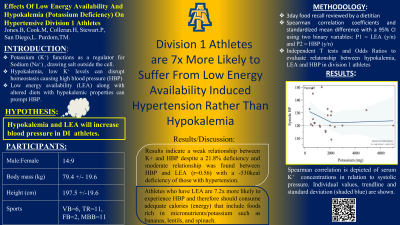
Potassium is an essential mineral that functions as a regulator for the human body. Adequate consumption of potassium aids in maintaining blood pressure by removal of sodium, which high sodium concentrations increase risk of developing hypertension. Potassium deficiency can occur during low energy availability (LEA) and is known as hypokalemia which can prompt the kidneys to reabsorb sodium back into the bloodstream increasing risk of hypertension. Potassium can be easily lost due to daily functions within the stool, respiration, and in athletes potassium can become deficient due to perspiration. However, there is limited research on how hypokalemia and its relationship to high blood (HBP) in athletes. PURPOSE: The purpose of this study is to investigate LEA and hypokalemia effect on cardiovascular health and HBP. METHODS: Subjects include 23 male and female division 1 athletes. Athletes' demographics were recorded with a wall mounted stadiometer (height) and bioelectrical impedance (body composition and weight). Athletes then rested for >5 minutes before blood pressure was taken with a sphygmomanometer according to The American College of Cardiology Heart Association classifications ( >120 - < 130 mmHg systolic BP and < 80 mmHg Diastolic BP). Presence of LEA and nutrient intake were measured by a Nutritional Data System for Research (NDSR) along with a food recall evaluated by a dietician. Total Energy intake (TEI) was calculated using the NDSR while energy expenditure (TEE) was estimated using the Shofield equation along with a physical activity level of 1.8 relevant to preseason to evaluate energy balance {Energy balance = TEI–TEE}. Statistical analysis included the Spearman correlation coefficients, standardized mean difference, independent T tests and Cohens D to evaluate the relationship between LEA and hypokalemia with elevated blood pressure in division 1 athletes using two binary variables: P1 =caloric deficiency (yes, no) and P2 = HBP (yes, no). Fisher’s exact test was used to find the value of P with significance set at (p < 0.05) RESULTS: A moderate relationship between LEA and HBP (R = 0.56; CI: 0.21, 0.90) was observed shown in Figure 1 with a -530kcal deficiency while no relationship with hypokalemia was observed (p > 0.05) despite a 21.8% deficiency in the HBP group. CONCLUSION: The LEA effect on physiological dysfunction contributed to HBP while the hypokalemia observed in the HBP group did not contribute to the negative hemodynamic function. PRACTICAL APPLICATION: Energy and nutrient deficiencies in athletes perpetuate nutrient deficiencies that contribute the HPB. Recommendations include consuming adequate calories to support meso/macro cycle goals along with a diverse food intake that are potassium rich such as: lentils, potatoes, bananas, and leafy greens.
Acknowledgements: Thank you to the NCAT Athletics Department for assisting us in the completion of this study