
Fitness/Health

Allison N. Wade
Graduate Student
Georgia Southern University- Armstrong
Tempe, Arizona, United States

Joe D. Vondrasek, CSCS
Graduate Student
Georgia Southern University
Savannah, Georgia, United States
Brian Oddi
Assistant professer
Pennwest California University
California, Pennsylvania, United States
Gregory J. Grosicki
Associate Professor
Georgia Southern University
savannah, Georgia, United States

Andrew A. Flatt, PhD, CSCS
Associate Professor
Georgia Southern
Savannah, Georgia, United States
Altered autonomic nervous system functioning is a hallmark of impaired recovery in athletes. Thus, resting heart rate (RHR) and its variability (HRV) are commonly used to monitor autonomic status in sports teams. Wearable devices support convenient HRV data acquisition via photoplethysmography, but many lack external validation.
Purpose: To evaluate the agreement between a commercially available wristband wearable device and electrocardiography (ECG) for determining RHR and HRV.
Methods: Twenty young adults (7 M/13 F, age = 22 ± 3 years, height = 168 ± 10 cm, weight = 71 ± 10 kg) volunteered for the study. For each subject, the wristband was placed on the left wrist per manufacturer instructions and paired with the mobile application on a tablet device via Bluetooth. A modified lead II configuration was used to collect RR intervals via ECG. The wearable device application offers a 2-min resting HRV assessment. Thus, 2-min recordings were simultaneously performed with the wristband and ECG in the supine followed by seated position. Recordings were preceded by ≥2 min for stabilization. RHR and the root-mean square of successive differences (RMSSD, a parasympathetic HRV index) were assessed. Criterion values were obtained from well-known HRV software with published RR processing algorithms.
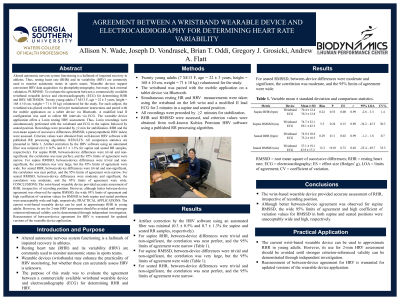
Results: All comparison statistics are presented in Table 1. Artifact correction by the HRV software using an automated filter was minimal (0.3 ± 0.5% and 0.7 ± 1.3% for supine and seated RR samples, respectively). For supine RHR, between-device differences were trivial and non-significant, the correlation was near perfect, and the 95% limits of agreement were narrow. For supine RMSSD, between-device differences were trivial and non-significant, the correlation was very large, but the 95% limits of agreement were wide. For seated RHR, between-device differences were trivial and non-significant, the correlation was near perfect, and the 95% limits of agreement were narrow. For seated RMSSD, between-device differences were moderate and significant, the correlation was moderate, and the 95% limits of agreement were wide.
Conclusions: The wrist-based wearable device provided accurate assessment of RHR, irrespective of recording position. However, although better between-device agreement was observed for supine RMSSD, the wide 95% limits of agreement and high coefficient of variation values for RMSSD in both supine and seated positions were unacceptably wide and high, respectively. PRACTICAL APPLICATIONS: The current wrist-based wearable device can be used to approximate RHR in young adults. However, its use for 2-min HRV assessment should be avoided until stronger criterion-referenced validity can be demonstrated through independent investigation. Reassessment of between-device agreement for HRV is warranted for updated versions of the wearable device application.
Acknowledgements: None