
Biomechanics/Neuromuscular
.jpg "Owen F. Salmon, MS photo")
Owen F. Salmon, MS
PhD Student / Research Assistant
Baylor University
Waco, Texas, United States

Matt Segovia, MS
PhD Student / Research Assistant
Baylor University
Waco, Texas, United States

Cierra Ugale, MS
PhD Student / Research Assistant
Baylor University
Waco, Texas, United States

Cory M. Smith, PhD
Assistant Professor
Baylor University
Waco, Texas, United States
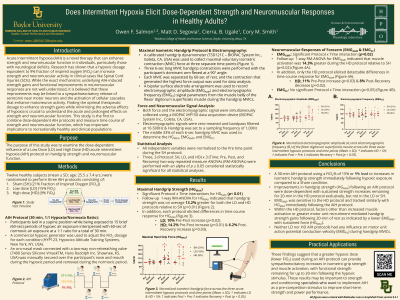
Purpose: Examine the dose-dependent influence of a Low Dose (LD) and High Dose (HD) acute intermittent hypoxia (AIH) protocol on hand grip strength and neuromuscular function.
Methods: Twelve healthy subjects (mean±SD age: 25.5±7.4 yrs) were randomized to perform three AIH protocols consisting of a Sham [SH] (21% Fraction of Inspired Oxygen [FiO2]), a LD (15% FiO2), and HD (9% FiO2) protocol. The AIH protocol consisted of 15 brief (60s) periods of hypoxic air exposure interspersed with 60s of normoxic air exposure delivered at a 1:1 ratio for 30-min using a hypoxic generator. Maximal isometric handgrip force (HGMAX) was recorded from the dominant hand, and surface electromyographic amplitude (EMGAMP) and frequency (EMGFC) were recorded from the flexor digitorum superficialis muscle of the same dominant arm. In addition, isometric hand grip strength (HGMAX), and neuromuscular activity were assessed before the AIH protocol (Pre), immediately following the AIH protocol (Post), and 20-min following the AIH protocol (Recovery [Rec]). All independent variables were normalized to the Pre time point during the SH condition. To assess changes in normalized force and normalized neuromuscular activity, four 3 (Condition: SH, LD, and HD) x 3 (Time: Pre, Post, and Rec) 2-way repeated measure ANOVAs (RM-ANOVAs) were performed.
Results: There were significant Protocol x Time interactions for HGMAX (p< 0.01), and EMGRMS (p=0.02), whereas, for EMGMPF there were no significant interactions or main effects for Protocol or Time. Follow-up 1-way RM-ANOVAs were performed for HGMAX, and EMGRMS across Protocols and Times. For HGMAX, there was a 10% Pre-Post increase following LD treatment (p=0.01), whereas, for the HD treatment, there was a 14.2% Pre-Post increase (p=0.02) and a 6.2% Post-Rec increase (p=0.03) observed. In addition, there were no significant differences in HGMAX across protocols during the Pre and Rec time points (p>0.05), however, during the Post time point, HGMAX was on average 13.2% greater in the LD and HD protocols compared to the SH (p< 0.01), with no differences observed between the LD and HD protocols. For EMGAMP there was an 11% Pre-Post increase (p=0.03) followed by an 8% Post-Rec decrease (p=0.01) during the HD protocol, with no differences observed during the LD or SH protocols. In addition, the HD protocol elicited a 14.3% increase in EMGAMP relative to the SH condition (p=0.02), with no detectable differences observed during the LD protocol or throughout the Pre or Rec time points.
Conclusion: These results suggest a dose-dependent increase in grip strength (HGMAX) from LD to HD compared to SH, with sustained strength increases remaining for 20-min following the HD protocol. In addition, EMGAMP, which reflects muscle activation, was sensitive to the HD protocol where muscle activation and grip strength tracked similarly following the HD protocol. However, grip strength remained elevated with a concomitant decrease in muscle activation following 20-min of Rec. PRACTICAL APPLICATIONS: These findings suggest that a greater hypoxic dose (lower FiO2) used during an AIH protocol can provide sympathoexcitatory increases in isometric grip strength and muscle activation, with functional strength remaining for 20-min following the hypoxic stimulus. These results may be important to strength and conditioning specialists who may want to implement AIH as a pre-competition stimulus to improve short-term strength and power performance.
Acknowledgements: None