
Body Composition

Casey J. Metoyer, MS, CSCS, SCCC
Sport Performance Associate
University of Notre Dame
Northport, Alabama, United States
.jpg "Katherine Sullivan, MS, ATC, LAT, USAW photo")
Katherine Sullivan, MS, ATC, LAT, USAW
Doctoral Candidate
University of Alabama
Tuscaloosa, Alabama, United States

Andrew D. Fields, MS, CSCS
PhD Student/Graduate Assistant
The University of Alabama - Tuscaloosa
Tuscaloosa, Alabama, United States
Michael V. Fedewa
Assocaite Professor
University of Alabama
Birmingham, Alabama, United States

Michael R. Esco
Professor
The University of Alabama - Tuscaloosa
Tuscaloosa, Alabama, United States
Introduction: The 4-compartment (4C) model is considered a criterion body composition method as it combines individual measures of body mass (BM), body volume (BV), total body water (TBW), and bone mineral content (BMC). However, this approach is not always feasible due to expense of equipment and the need for trained personnel. Bioelectrical impedance analysis (BIA) is a common, portable, low-cost technique to assess body composition. However, the ability of BIA to predict both TBW and BMC within a 4C model has yet to be examined.
Purpose: The purpose of this study was to determine the accuracy of an experimental 4C model (4CEXP) utilizing bioimpedance based TBW and BMC to a criterion 4C model (4CCR) when BV measures were held constant.
Methods: Participants (n=42, 71% female, (25.0±7.9 years, 169.9±8.1 cm, 72.9±16.9 kg) completed a single visit to the Exercise Physiology Laboratory at the University of Alabama. Standing height was measured to the nearest 0.1 cm using a stadiometer (SECA 213, Seca Ltd., Hamburg, Germany). Body mass was measured to the nearest 0.1 kg using a calibrated digital scale (Tanita BWB-800, Tanita Corporation, Tokyo, Japan). Dual-Energy X-Ray Absorptiometry (DXA) was used to calculate BMC for the 4CCR. Hand-to-foot bioimpedance spectroscopy (ImpTM SFB7, ImpediMed Limited, Queensland, Australia) was used to determine TBW, with built-in algorithms, for the 4CCR. Whereas a single frequency (50 kHz) hand-to-foot BIA device (Quantum iV, RJL Systems Inc., Clinton, MI) was used to determine TBW and BMC for the 4CEXP. Underwater weighing (UWW) was completed and used to calculate body volume for both 4C models. Residual lung volume was determined using the oxygen dilution technique via nitrogen analysis (ParvoMedics True Max 2400; ParvoMedics, Sandy, UT) while in a seated position immediately prior to the UWW procedure. The potential difference between the %Fat estimate was assessed using a paired samples t-test, with a Cohen’s d effect size used to describe the observed error as small, moderate, or large (d=0.2, 0.5, and 0.8, respectively). The association between %Fat estimates was assessed using Pearson’s r correlation coefficient and described as weak, moderate, strong, and nearly-perfect (r=0.2, 0.5, 0.8, and 0.9, respectively). The corresponding standard error of the estimate (SEE) was described as good, excellent, or ideal (SEE=3.0, 2.5, and < 2.0 %Fat, respectively).
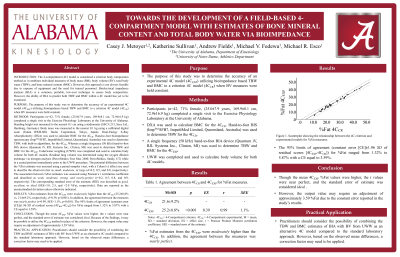
Results: %Fat estimates from the 4CEXP were moderately higher than the 4CCR (25.2±8.8% vs. 21.6±9.2%, respectively, d=0.39, p< 0.001). In addition, the agreement between the measures was nearly perfect (r=0.99, SEE=1.1%, p< 0.001). The 95% limits of agreement (constant error [CE]±1.96 SD of residual scores [4CBIA-4CCR]) for %Fat ranged from 1.32% to 5.87% with a CE equal to 3.59%.
Conclusion: Though the mean 4CEXP %Fat values were higher, the r values were near perfect, and the standard error of estimate was considered ideal. Because of the findings, it may be possible to utilize the 4CEXP method in place of the criterion. However, the output value may require an adjustment of approximately 3.59 %Fat.
PRACTICAL APPLICATION: Practitioners should consider the possibility of combining the TBW and BMC estimates of BIA with BV from UWW as an alternative 4C model compared to the standard laboratory approach. However, based on the observed mean differences, a correction factor may need to be applied.
Acknowledgements: None